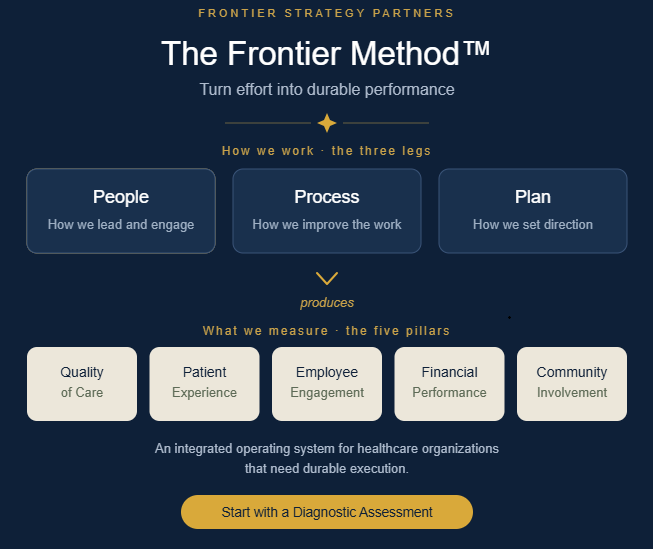
The Frontier Method™ - Turning Effort Into Durable Performance in Healthcare
Walk into almost any healthcare organization and you will find people working hard. Leaders are stretched across more responsibilities than the calendar can hold. Staff are giving more than the staffing model assumes. Boards are asking serious, well-informed questions. Dashboards are full of data. Strategic plans exist, often handsomely bound, and improvement projects are underway in half a dozen departments. And yet, in organization after organization, the same problems keep coming back. Strategic plans live in a binder while daily operations run on instinct. Improvement efforts launch with energy and quietly fade. Engagement surveys surface the same frustrations year after year, and the issues they name go unresolved. Quality, finance, patient experience, workforce, and community priorities are each reviewed in their own meeting, by their own committee, on their own cadence, rarely in the same room and almost never as one connected story.
The gap is not a gap in effort. It is a gap between effort and durable performance, and that is the gap the Frontier Method was built to close.
The Frontier Method is a management system for healthcare organizations that need durable execution. Rather than adding one more initiative to an already crowded agenda, it integrates the disciplines most organizations already practice, including leadership and engagement, process improvement, strategic planning, performance measurement, and board oversight, into a single coherent operating rhythm. The simplest way to express its value is this: the Frontier Method helps healthcare organizations turn leadership effort, improvement work, strategic planning, and performance measurement into one integrated operating system.
We want to be honest about what is and isn't novel here. The Method does not claim that rounding, Lean, A3 problem solving, daily huddles, strategic planning, scorecards, or board reporting are new ideas. Each of these is well established. Our contribution is the integration of these familiar disciplines into one healthcare specific operating system, so that they reinforce one another instead of competing for attention in separate lanes.
Differentiation Isn't a Feature List: Using Playing to Win to Operationalize Porter in a Rural Hospital
There is a familiar exercise that plays out in hospital boardrooms across rural America. A consultant or a new CEO gathers the leadership team and asks what makes the hospital different. The flip chart fills up quickly: we know our patients by name, we have great nurses, we're committed to the community, we offer compassionate care, we're investing in technology, we're recruiting new specialists. Everyone nods. The list goes into the strategic plan. A year later, margins are worse, the regional system across the county line has bought another physician practice, and nobody can quite explain why the strategy isn't working.
The reason is that almost nothing on that flip chart is strategy. It is, in Michael Porter's terms, a description of operational effectiveness wearing strategy's clothes. And it is precisely the trap that independent rural hospitals fall into when they try to compete with regional systems by becoming smaller, friendlier versions of them.
This post is about how to escape that trap. It combines two of the most useful frameworks in modern strategy, Michael Porter's 1996 essay What Is Strategy? and A.G. Lafley and Roger Martin's Playing to Win (2013), and applies them to one of the hardest strategic environments in American business: the independent rural hospital. The focus throughout is on differentiation, because differentiation is where Porter is sharpest, where rural hospitals are most confused, and where the combination of these two frameworks does its best work.
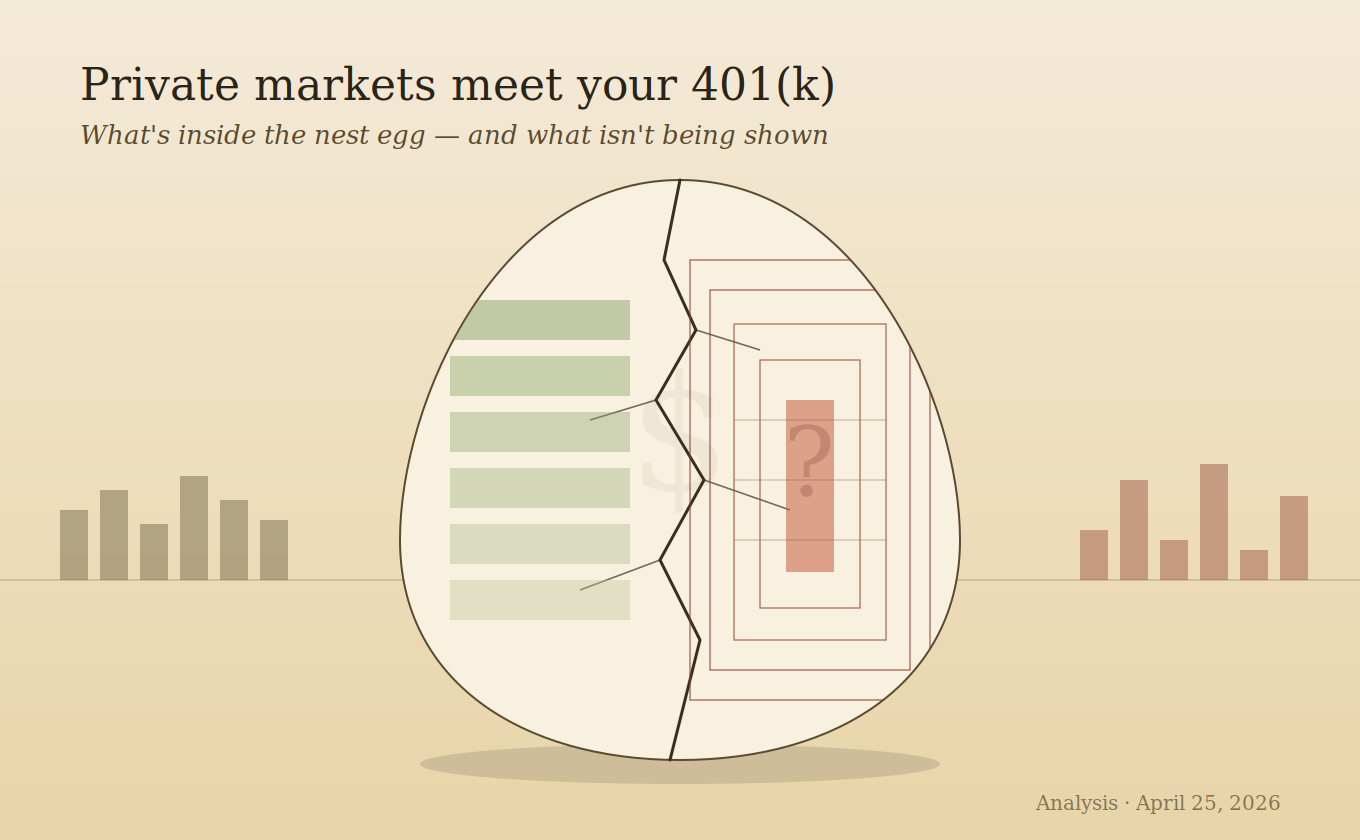
Private Markets and Your 401(k) - What You Need to Know Right Now
Washington just proposed opening your 401(k) to private equity and private credit. Supporters say it will give ordinary workers access to returns that have long been reserved for the wealthy. Critics say it will expose retirement savers to opaque, illiquid, and overvalued assets at the worst possible moment. Both sides have a point. This piece tries to lay out what each side gets right, what each side omits, and what you would need to know to make an informed decision if these options show up in your retirement plan.
HOW WE GOT HERE
The private credit market grew from a niche corner of finance into a $1.8 trillion industry over the past decade, fueled by low interest rates, a shrinking universe of public companies, and banks retreating from leveraged lending after post-2008 regulation. Firms like Apollo, Blackstone, Ares, and Blue Owl stepped into the gap, making high-interest loans to private equity-backed companies — many of them software businesses — and offering wealthy individuals access to yields unavailable in public markets.
For a long time, it worked well. Private equity returned 15.1% annually on average between 1984 and 2024, versus 11.7% for the S&P 500. University endowments like Harvard's put 77% of their portfolios into private and alternative investments. Government pension funds allocated roughly a third of their assets to alternatives. The returns were real, and the institutions that earned them were sophisticated, long-term investors with professional staff and full transparency into what they owned.
That context matters for everything that follows.
The Playing-to-Win Strategy Canvas - A Practical Guide for Rural Hospital Leaders (Part 2)
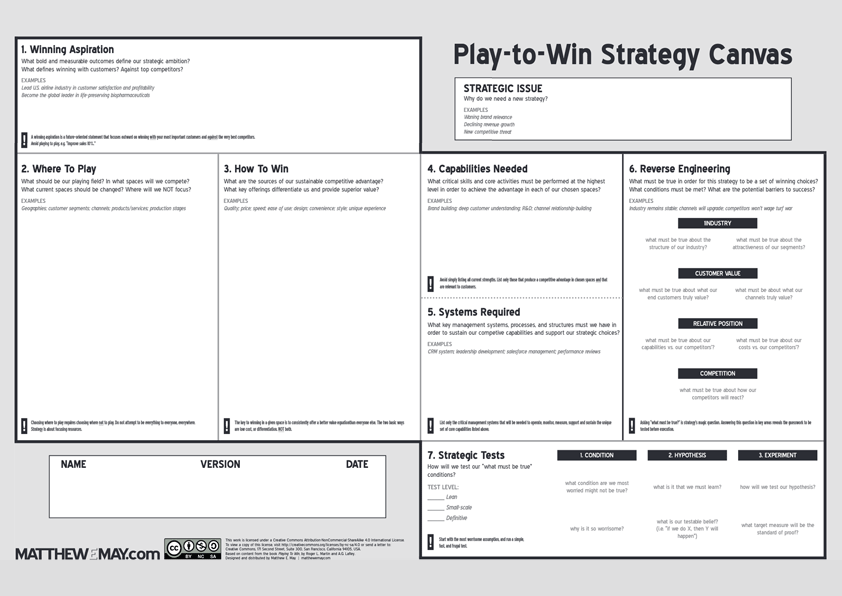
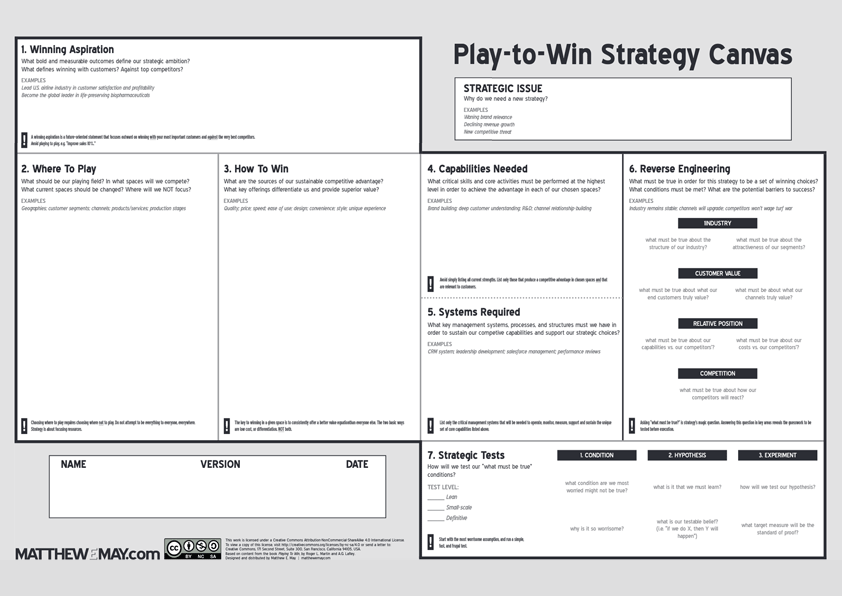
In Part 1, we walked through the Choice-Making stage of Matthew E. May's Playing-to-Win Strategy Canvas — the five interconnected elements that define your strategic position: Strategic Challenge, High-Level Option, Winning Aspiration, Where to Play, and How to Win, supported by Critical Capabilities and Required Systems.
If you stopped there, you'd already have a more rigorous strategy than most hospital strategic plans produce. But the Canvas doesn't stop there — and neither should you.
The real power of this framework lives in what comes next: two stages that force you to pressure-test your strategy before committing scarce resources. For Critical Access Hospital leaders managing 25-bed operations with limited capital and no margin for strategic error, these stages aren't optional. They're where you separate conviction from wishful thinking.

The Water Is Rising - What Every Leader Needs to Understand About AI Right Now
Think back to February 2020. You were probably going about your normal life — going to restaurants, shaking hands, planning trips. Maybe you had seen a headline or two about a virus spreading overseas, but life felt normal. It was normal. And then, over the course of about three weeks, everything changed. Schools closed. Offices emptied. The world rearranged itself into something you wouldn't have believed if you had described it to yourself a month earlier.
Matt Shumer, CEO of OthersideAI and a six-year veteran of the AI startup world, opens his February 2026 essay "Something Big Is Happening" — which has now been viewed by more than 50 million people in less than a month — with exactly that image. "I think we're in the 'this seems overblown' phase of something much, much bigger than Covid," he writes. That framing is worth sitting with. Not to induce panic, but because the alternative to understanding what is coming is being defined by it rather than shaping your response to it.
I'm not writing this as a technology enthusiast. I'm writing this as a healthcare executive and strategic advisor who has spent more than two decades working in environments where resources are constrained, change is constant, and the margin for error is thin. The leaders I work with are smart, experienced, and deeply committed to the people and communities they serve. Most of them have heard about AI. Many have experimented with it casually. Almost none of them have reckoned with what is actually happening right now — and what it means for them, their organizations, and the people who depend on them.
This piece draws on two remarkable works published in early 2026: Shumer's blog post and Howard Marks' February 26 memo "AI Hurtles Ahead" from Oaktree Capital Management. Together, they offer something rare: the urgency of a practitioner experiencing the shift in real time, paired with the measured analytical discipline of one of the most respected investors of the past half century. My goal is to synthesize their insights and translate them into something actionable for leaders operating in any sector — healthcare, finance, law, manufacturing, education, and beyond.
The Playing-to-Win Strategy Canvas - A Practical Guide for Rural Hospital Leaders
Let's be honest about something most of us already know but rarely say out loud: the vast majority of hospital strategic plans are exercises in aspiration, not strategy. They produce beautifully formatted documents that sit in binders and on SharePoint sites, referenced during board meetings and forgotten everywhere else. For rural and Critical Access Hospitals operating with razor-thin margins and shrinking workforces, this isn't just wasteful — it's dangerous.
The problem isn't a lack of effort. It's a lack of framework. Most strategic planning processes in healthcare are built on tools designed decades ago for fundamentally different environments. SWOT analyses, for all their ubiquity, produce inventories of observations rather than actionable choices. Balanced scorecards measure execution of existing strategy but don't generate new strategic insight. And visioning exercises, while energizing in the moment, often produce aspirations disconnected from the hard choices required to achieve them.
There is a better way. The Playing-to-Win Strategy Canvas, developed by Matthew E. May and built on the foundational strategic framework from A.G. Lafley and Roger Martin's Playing to Win: How Strategy Really Works, is a single-page tool that forces the kind of rigorous, integrated thinking that separates real strategy from strategic theater.
This is Part 1 of a two-part series. Here, we'll walk through the Canvas's first stage — Choice-Making — with practical examples that reflect the realities Critical Access Hospital leaders face every day. In Part 2, we'll cover Reverse Engineering and Barrier Testing, the stages that stress-test your strategy before you commit scarce resources.
Leveling the Playing Field to Close the $40 Million Gap Threatening Rural Hospital Districts
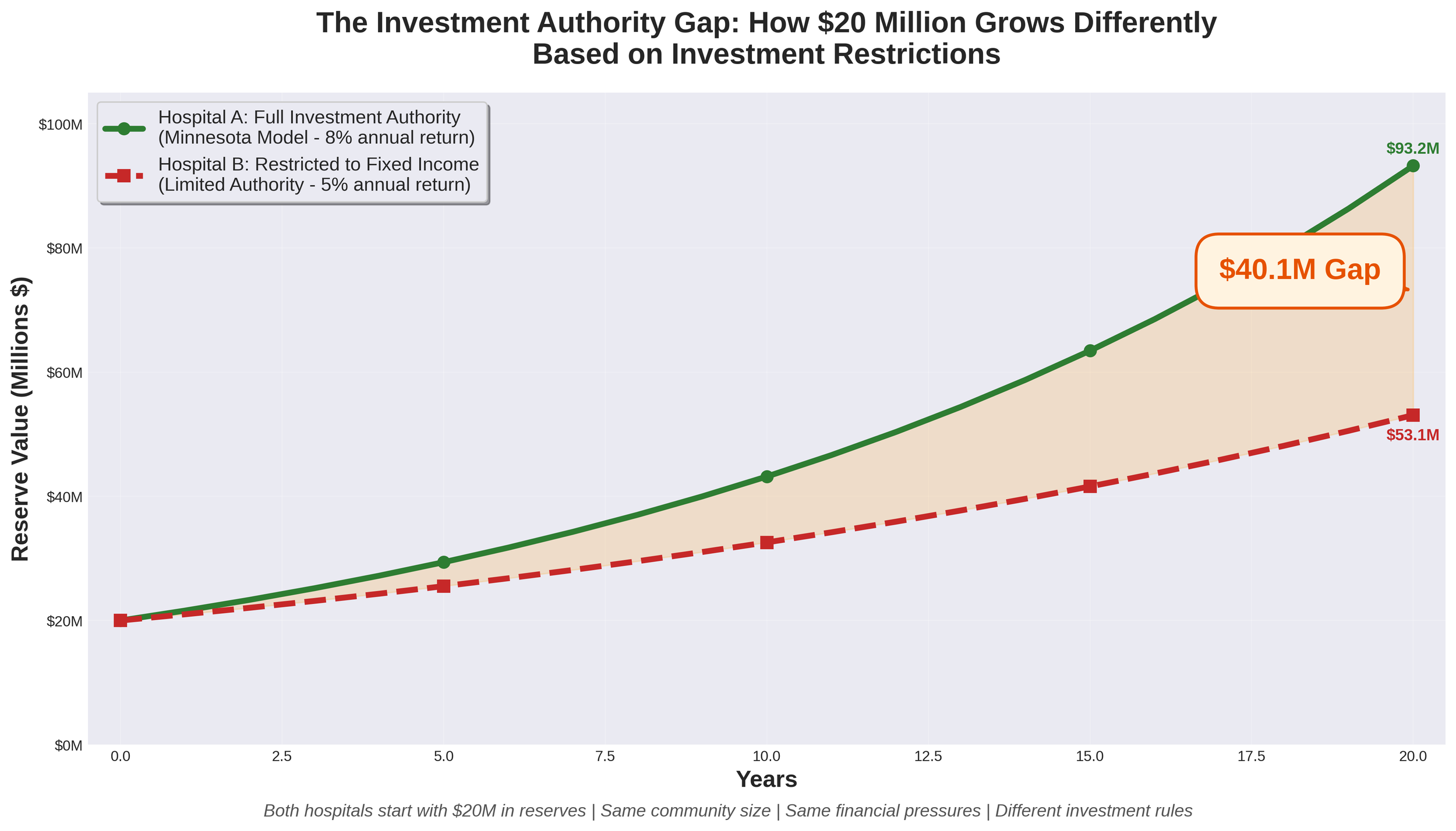
Imagine two nearly identical Critical Access Hospitals in neighboring states. Both serve rural communities of approximately 11,000 residents. Both have worked hard to build $20 million in reserves to weather financial storms and invest in their futures. Both face the same financial headwinds threatening rural healthcare nationwide.
There's just one critical difference: One hospital can invest its reserves like every other non-profit healthcare organization in America. The other cannot.
Twenty years later, the first hospital has grown its reserves to approximately $93.2 million. The second hospital has barely $53.1 million. That $40 million gap represents the difference between survival and closure for a rural community.
Rural hospitals across America are facing unprecedented financial pressures. More than 180 rural hospitals have closed nationwide since 2005, and the trend is accelerating. The challenges are well-documented: Medicare and Medicaid reimbursement rates that don't cover the cost of care, rising levels of uncompensated care as insurance coverage gaps widen, workforce shortages requiring premium compensation to recruit and retain staff, healthcare-specific inflation that outpaces general inflation (particularly for labor, pharmaceuticals, and supplies), escalating technology and cybersecurity costs, and increasing regulatory demands.
For hospital districts across many states, these universal challenges are compounded by a structural disadvantage that few people understand: constitutional or statutory restrictions that prevent them from competing on a level playing field with private non-profit hospitals. While private 501(c)(3) hospitals can invest their reserves in diversified portfolios including equities, many governmental hospital districts remain restricted to low-return fixed-income investments. This gap in investment authority creates a compounding disadvantage that threatens the long-term viability of publicly-owned rural hospitals.
Let's examine this issue using Nebraska as a case study—but the implications extend to hospital districts in any state facing similar investment restrictions.

An Open Letter to Tyson Foods Leadership
My name is Jason Douglas, and I serve as CEO of Lexington Regional Health Center, a Nebraska Hospital District, here in Lexington, Nebraska. I came to this community in March of this year as a healthcare administrator who passionately believes in the mission of serving rural communities. I'm writing to you as someone who has spent the past two weeks watching families in our community try to find their footing after your November 21st announcement.
You gave them a Friday afternoon, right before Thanksgiving. It'll be memorable, as November 21st just happened to be my birthday. I'd planned to spend it settling further into this community I'd grown to love and appreciate in my short time here. Instead, I spent it fielding calls and beginning to understand the scope of what your decision would mean for the people I came here to serve.
What matters is that 3,200 people learned that same day their jobs would be gone by January 20th—then went home to prepare a holiday meal with their families. To sit across the table from their children and try to find something to be thankful for. To lie awake that night doing math in their heads—how many paychecks left, how long until insurance runs out, whether they can make rent in February.
That was your timing. That was your choice.

2025 Rural Healthcare Year in Review - When Rhetoric Met Reality
The year 2025 will be remembered as the moment rural healthcare advocates learned to read between the lines of political theater. It began with Robert F. Kennedy Jr.'s confirmation hearings for HHS Secretary, where nearly every senator—Republican and Democrat alike—stressed the critical importance of preserving healthcare access and coverage in rural America. It ended with rural hospitals facing the largest federal healthcare cuts in Medicaid's history, a marketplace subsidy cliff that may never be resolved, and a "transformation grant" that delivers a fraction of what the rhetoric promised.
The question we must ask: Do the policies enacted in 2025 support the narrative presented during Kennedy's confirmation, or do they expose it as empty posturing?

The $100,000 H-1B Fee - A Policy That Undermines American Competitiveness
The recent decision to impose a $100,000 fee on new H-1B visa applications represents a fundamental misunderstanding of how global talent drives American economic success. While framed as protecting American workers, this policy will likely harm both American competitiveness and the very workers it claims to help.
America's dominance in technology, healthcare, and innovation has been built on a simple principle: attract the world's best talent and let them create value here. This policy abandons that winning strategy for a fundamentally flawed premise that high-skilled immigration is a zero-sum game. The $100,000 fee effectively transforms H-1B visas from a workforce tool into a luxury good. For a medical resident earning $55,000 annually, no hospital will rationally pay twice their salary just for the privilege of hiring them. For a brilliant recent PhD who might revolutionize artificial intelligence or develop life-saving treatments, the fee creates an arbitrary barrier that has nothing to do with their potential contribution to America.

Strengthening Rural Healthcare - Understanding the Nebraska High Value Network and Value-Based Care
On June 5, 2025, the Nebraska High Value Network (NHVN) officially launched with 19 critical-access hospitals joining forces to strengthen healthcare delivery across rural communities. This collaborative network, organized by Cibolo Health, represents more than just a partnership—it's a strategic approach to ensuring sustainable, high-quality healthcare remains accessible in rural Nebraska.
The network's cornerstone is a clinically integrated network (CIN) that will serve nearly 300,000 patients while allowing each hospital to maintain its independence and community focus. For healthcare leaders like myself, this model offers a compelling path forward in an increasingly complex healthcare landscape.

The Future of Medicine - How AI and Quantum Computing Are Revolutionizing Drug Discovery and Patient Care
We stand at the threshold of a medical revolution. While the promise of personalized medicine has tantalized researchers for decades, we're finally seeing the convergence of technologies that can deliver on that promise at scale. Leading this charge is an unlikely partnership between a century-old Danish pharmaceutical company and cutting-edge quantum computing research—a collaboration that's rewriting the rules of drug discovery and patient care.
Novo Nordisk, best known for its diabetes treatments and the blockbuster obesity drug Wegovy, has quietly become one of the most innovative forces in computational medicine. Their recent breakthroughs offer a glimpse into a future where artificial intelligence doesn't just assist doctors—it fundamentally transforms how we understand, predict, and treat disease.

Leadership Perspectives - Navigating the Nuances of Authority and Influence
We're excited to welcome Jess Nuutinen back to our leadership series with her insightful exploration of the critical distinction between being a boss and being a leader. Following her previous contribution on shared governance, Jess now turns her analytical lens to the subtle yet profound differences that separate positional authority from true leadership. In "Boss vs. Leader: Understanding the Key Differences," she skillfully dissects how these contrasting approaches affect team dynamics, organizational culture, and long-term success. Jess's thoughtful examination of authority versus influence, task-orientation versus people-orientation, and control versus empowerment provides valuable guidance for healthcare professionals at every level. Her practical wisdom reminds us that effective leadership transcends titles and hierarchies—a timely message that complements our growing collection of leadership perspectives. As you read her compelling analysis, we invite you to reflect on your own leadership style and consider how you might incorporate more leadership qualities into your daily practice.

Transformative Leadership - Making a Meaningful Difference
We're pleased to continue our leadership series with an enlightening contribution from Dan Swenson that challenges conventional notions of leadership. In "Transformative Leadership - Making a Meaningful Difference," Dan thoughtfully explores how true leadership transcends formal titles and hierarchies to focus on creating genuine impact. His perspective offers a refreshing counterpoint to authority-centric leadership models, emphasizing instead how service, compassion, and humility form the foundation of transformative leadership. Dan's insights are particularly relevant in healthcare settings, where leadership decisions directly affect patient outcomes and organizational culture. As Frontier Strategy Partners continues to showcase diverse leadership philosophies, Dan's emphasis on accessible leadership—available to everyone regardless of position—adds a valuable dimension to our ongoing conversation. His message that leadership is ultimately measured by positive impact rather than power aligns perfectly with our commitment to exploring leadership approaches that create lasting, meaningful change.

Building Excellence in Healthcare Through a Comprehensive Management System
Exceptional performance is rarely achieved through isolated initiatives or the heroic efforts of individuals. Instead, sustainable excellence requires a comprehensive management system that aligns people, processes, and strategic direction. Having observed this healthcare transformation effort, I've become convinced that the "three-legged stool" approach—integrating People, Process, and Plan—offers a powerful framework for healthcare organizations seeking to elevate performance across all dimensions.

Leadership Perspectives - The Critical Role of Non-Clinical Leadership in Healthcare Excellence
We're excited to continue our leadership series with a compelling contribution from Kevin Stranberg of Stranberg and Associates. In this insightful piece, Kevin illuminates the often-overlooked yet essential role that non-clinical leadership plays in creating exceptional healthcare experiences. Building upon the shared governance principles explored in Jess Nuutinen's previous article, Kevin expertly demonstrates how non-clinical departments form crucial pillars in a healthcare organization's cultural foundation. His holistic perspective reminds us that exceptional patient care depends on every team member—from registration to housekeeping—working in concert toward a common mission. Kevin's thoughtful analysis of empowerment, collaboration, and accountability across departmental boundaries reflects his deep understanding of healthcare systems and organizational dynamics. We're confident his wisdom will provide valuable insights for leaders throughout your organization, regardless of their clinical or non-clinical roles.
Strong leadership in non-clinical departments of the healthcare system is essential to overall success. Although most clinical departments generally have limited direct contact with patients, their efforts are important components of the overall culture of the organization. Time and time again when patients are asked the question “did staff work together to care for you?” they include everyone they have come in contact with during their visit – registration, housekeeping, nutrition, patient financial to name a few. As a leader of non-clinical staff, the focus of the work needs to be clear and important to every staff. This focus centers on many of the same priorities listed by Jessica Nuutinen in the previous leadership article on Shared Governance – Empowering Healthcare Teams Through Collaborative Leadership for clinical staff leadership.

Shared Governance - Empowering Healthcare Teams Through Collaborative Leadership
In our continuing leadership blog series, we're pleased to feature Jess Nuutinen's insightful exploration of shared governance—a cornerstone concept in modern healthcare leadership. Jess brings a wealth of experience to this topic, offering a thoughtful analysis of how collaborative decision-making transforms healthcare organizations. As Frontier Strategy Partners continues to examine diverse leadership approaches, Jess's perspective highlights how distributing authority and responsibility across all levels of healthcare professionals creates more resilient, innovative, and patient-centered organizations. Her practical framework for implementing shared governance reflects our commitment to providing actionable leadership strategies that can be applied across various healthcare settings. Join us as Jess illuminates this powerful approach that bridges the gap between frontline caregivers and organizational leadership.
Shared governance is a vital framework in health care and nursing that promotes collaboration, accountability, and empowerment among nursing staff and other health care professionals. By fostering a participative decision-making process, shared governance allows nurses to have an active role in shaping policies, procedures, and practices that directly impact patient care and workplace dynamics.

The A3 Approach - A Practical Guide to Strategic Documentation in Healthcare
Organizations face unprecedented challenges that demand focused strategic responses. Yet many healthcare institutions struggle with strategic clarity—developing plans that are unwieldy, difficult to communicate, and even harder to implement effectively. The A3 methodology offers a powerful solution to this common challenge.
Originally developed by Toyota as part of their lean management system, the A3 approach has found remarkable resonance in healthcare settings. Taking its name from the international paper size (11x17 inches) that serves as its canvas, this methodology constrains strategic documentation to a single page—forcing clarity, precision, and prioritization.

Measuring Success Through Strategic Pillars
Delivering sustainable results requires more than just setting broad organizational targets. True success comes from creating a comprehensive system where every aspect of the hospital, from executive leadership to individual departments, aligns its efforts with a unified purpose. At the heart of this alignment lies a structured approach to goal setting that ensures the organization moves forward cohesively toward its mission and vision.
The strategic pillar framework offers healthcare organizations a powerful methodology to measure success across critical operational areas. By organizing goals around five foundational pillars—Quality, Workforce, Patient Satisfaction, Finance, and Community—hospitals create clear pathways for improvement while ensuring that priorities cascade effectively throughout all levels of the organization.

The Strategic Impact of Communication on Organizational Success
Communication stands as the foundational element that shapes organizational culture and drives employee engagement. Far beyond the simple exchange of information, strategic communication serves as the invisible architecture that aligns teams, builds trust, and propels organizations toward their goals.
Successful organizational communication hinges on three critical dimensions: the message content, the delivery mode, and the target audience. When these elements are strategically aligned, communication transforms from a mundane operational function into a powerful catalyst for organizational cohesion and performance.